You need more than a little patience to deal with a lengthy dental procedure. You need to understand why each step is important and why it led to the next one. You can’t do this if you don’t get the facts straight about dental treatment plans. Otherwise, each appointment can feel like an isolated event rather than part of a coherent whole. The more you understand the reasoning behind the sequence, the easier it becomes to stay committed when the process runs long.
Demystifying The Multi-Phase Treatment Plan
When a dentist proposes something like full-mouth rehabilitation, implants, or a combination of crowns and gum treatment, patients often feel like they’ve been handed a roadmap to a country they’ve never visited. The sequencing can seem arbitrary, especially when you’re asking why you can’t just get the new crown now instead of spending three months on gum therapy first.
The structure exists for good clinical reason. Complex dental rehabilitations typically move through four phases: diagnostic, preparatory, corrective, and maintenance. Diagnostic comes first – this is where advanced imaging like dental cone beam CT (CBCT) gives the clinical team a three-dimensional picture of bone density, nerve positions, and the structural landscape they’re working within. Preparatory addresses anything that would undermine downstream work: periodontal disease, active infections, or inadequate bone volume. Corrective is where the visible restorative work happens – implants, crowns, bridges. Maintenance is everything after.
Trying to skip from diagnostic to corrective is like laying hardwood floors over a waterlogged subfloor. The work will fail, and it’ll cost more to fix than doing it right the first time would have.
Dental Hygiene As The Foundation – Not The Footnote
Many patients don’t realize the importance of this aspect. It’s not just something you do before the actual treatment. It’s the determining factor of whether all the expensive work will be successful or not.
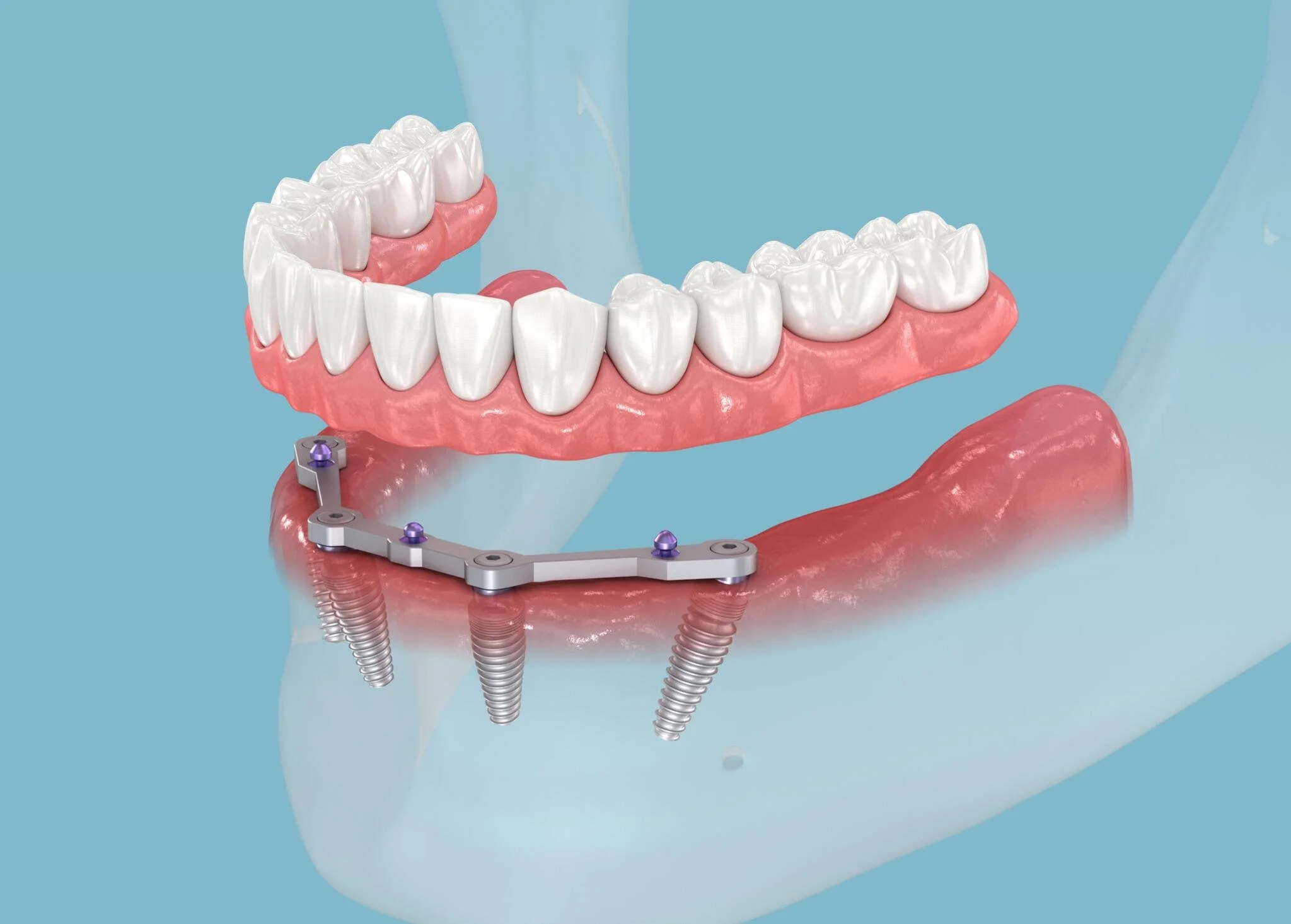
Take dental implants. Their success relies on osseointegration, the process by which the jawbone fuses to the titanium post over several months. This is highly vulnerable to bacterial activity. If a patient has uncontrolled plaque, subgingival calculus, or active periodontal disease upon the placement of an implant, the likelihood of peri-implantitis, a devastating infection in the space left by the implant, rises considerably. Patients without a professional dental hygiene schedule after their implant therapy fail at a rate nearly three times that of those who adhere to one – 9.0% versus 3.0% across ten years (Journal of Clinical Periodontology).
Bone grafts are similarly dependent on a sterile, healthy tissue environment. And for root canal therapy, the short- to long-term success of the restoration crowning the treated tooth is closely linked to postoperative hygiene around it.
Gingivitis is the warning sign. It is reversible, but it indicates to the clinical team what your daily home care really involves. If gingivitis persists into the pre-operative phase, that’s a warning signal before any surgical work is undertaken.
It’s not background noise. It’s the floor joist.
Evaluating A Proposed Treatment Plan Before You Agree
Informed consent is a dry term, but the truth is, most people trustingly listen to the treatment plan, sign the dotted line and go through the motions.
Here are the plain questions to ask before you accept complex treatment:
What’s the alternative? In most restorative conditions of the mouth, there’s a different treatment option. You need to be aware of the alternative route so you take your decision with your eyes open.
What material and why? Zirconia crowns are not the same as porcelain fused to metal crowns. They differ in looks, strength, and cost as well. Be sure to ask what is being recommended and why these are suitable for you.
What’s the lifespan (low and high) you have noticed with this treatment modality? Every dentist knows approximately how long a bridge or implant is expected to be functional. Instead of general answers, your dentist should give you a range.
What happens if I postpone a phase? You should know if postponing Phase 2 implant after Phase 1 extraction is a good choice or might it cause serious bone loss and additional cost in future treatment.
Choosing The Right Clinical Team
Not all dental practices are equipped to provide multi-phase treatment that encompasses both surgical needs and long-term hygiene maintenance. However, patients can generally expect safer, more predictable outcomes from practices that can handle the full scope of diagnostics, treatment, and recovery since the restorative and hygiene teams in those practices share every detail.
A team like Mandurah Dental Surgery, for example, is configured to ensure that patients have continuous support of this kind; the hygienist they’d see for regular maintenance cleanings post-treatment would already be fully aware of their surgical history.
When you’re in a chair looking for advice about complex care planning and looking at who to trust, you might want to ask where they’d send you for hygiene maintenance phase work after your treatment is complete. If the answer is that they don’t handle it, it’s something to think about.
Pre-Treatment Preparation: What To Do In The Weeks Before Surgery
The time between agreeing on a treatment plan and actually having surgery can be a time of high anxiety… but also of high clinical importance. What patients do or don’t do in this time frame can have a dramatic effect on intraoperative and post-operative outcomes.
Just as you might receive a prescription for chlorhexidine oral rinses in the days prior to your surgery, to help reduce the bacterial load in your mouth and lower your risk of intraoperative bacteremia, non-adherence to that prescription isn’t a victimless error. Use them as directed, not just occasionally.
If an implant or bone graft is in your future, smoking cessation is non-negotiable. The vasoconstrictive properties of cigarettes suppress the vascular supply necessary for healing in these contexts. But “cutting down for upcoming surgery” isn’t really a thing either: even cutting back doesn’t cut it. It’s quitting for several weeks in advance of the procedure and for the full period of healing after the surgery that makes a clinical difference in outcomes.
If you have xerostomia (dry mouth), whether from medication or another cause, tell your dentist before treatment begins. Dry mouth removes saliva’s natural antimicrobial and buffering functions, which increases decay risk and slows soft tissue healing. There are targeted management strategies, but the team needs to know about it.
Achieving stable gum health before surgery is the most important preparatory step. That means professional prophylaxis to remove subgingival calculus, and genuine improvement in daily interdental cleaning – floss, interdental brushes, or water flossers used consistently, not just the week before your appointment.
Post-Operative Hygiene For Complex Restorations
After surgery, the way you brush has to be different. The force that’s needed for maximum cleaning effect in a normal situation, for example, when you’re cleaning an implant site, a bone graft, or a temporary crown, can be too much for the weakened clot that’s trying to establish itself, the weaker bond of the provisional restoration, or the vulnerable open wound.
With implant sites, the general guideline is to avoid direct brushing and use instead a rinse of chlorhexidine or saline to keep the site as clean as possible in the first days post-op. As tissue starts healing, you’ll be ready to reintroduce the brush – an extraordinarily soft brush, using the minimum of pressure.
Temporary crowns and bridges can easily be dislodged by the normal brushing action. They’re only seated with provisional cement to make sure they can be removed when the time comes. Lateral pressure will pop them off. Floss around temporaries carefully – thread it through rather than snapping it under the contact – and avoid hard or chewy foods. Use a floss threader or just the loose end of the floss.
The healing phase for osseointegration typically runs three to six months. Throughout that period, every visit to the hygienist is an opportunity to monitor the site and catch any early signs of peri-implantitis before it progresses.
Managing Information Overload And Dental Anxiety
Treatment plans that are complicated can be overwhelming. You don’t just get the information that you need a root canal, you learn your tooth needs a root canal, a post, and a crown, and you also need a deep cleaning and two fillings. Now you must somehow manage all that.
If the language of dentistry is Greek to you, and you can’t hold up the illusion otherwise, start by asking your provider for basic, less stressful explanations of everything. Most staff are happy to oblige and will pull out more easy-to-understand models or charts.
Breaking it into several smaller procedures to declutter the docket might be a good option if your practice can accommodate that. You feel less overwhelmed with two things tomorrow, five things next week, and six in 2 weeks than you do with thirteen things suddenly hanging over your head.
If anxiety is severe enough to interfere with procedures themselves, ask about sedation options. These exist on a spectrum from oral sedation to IV sedation, and they’re a legitimate part of complex treatment planning, not a last resort.
Long-Term Maintenance Is The Real Treatment
It is a misconception that you go through the effort of such a complex plan only to be “done”. It is the beginning of the next phase, the Maintenance Phase. That lasts as long as you wish to keep your investment.
Prosthodontic restorations (crowns, bridges, implant supported prosthetics) require professional monitoring based on the specifics of your case. These appointments aren’t optional check-ups – these are where low-grade problems are identified and dealt with, allowing repair instead of repeating the need for intervention.
Your home care kit will also likely change. You may still use regular floss but it will likely be supplemented by a water flosser, superfloss, or special interdental brushes that are appropriately sized for you. Your hygienist should help adapt these suggestions for you.
Financing Complex Treatment Without Compromising Outcomes
Let’s talk about the cost of complex dental work. It’s not cheap, and we’re not doing ourselves or our patients any favors by skirting directly around that uncomfortable truth. However, it’s also true that in terms of health economics, good dentistry is a solid proposition. It’s durable, preventative, and able to stave off some really significant health problems down the line.
One way to amortize the investment over time is to phase the treatment. By phasing major dental work across two separate calendar years, you can essentially double the benefits available for two major episodes of treatment. This can be a significant up-front saving for many patients and greatly assists with budgeting for the second part of their treatment.
Most practices offer payment plans or work with third-party financing. Ask for an itemized treatment schedule with costs per phase so you can have a real conversation about sequencing based on both clinical priority and financial capacity.
What’s worth resisting is the temptation to skip the preparatory phase to get to the visible restorative work faster. Skipping periodontal treatment to proceed directly to implants, for example, almost always costs more in the long run – financially and clinically. The phases exist because the sequence matters.
Complex dental treatment done well is one of the more durable investments a person can make in their health. The patients who come through it with the best outcomes aren’t necessarily those with the most straightforward cases – they’re the ones who understood what was being asked of them and followed through.